An e-publication by the World Agroforestry Centre
INDIGENOUS KNOWLEDGE OF
MEDICINAL TREES AND SETTING PRIORITIES
FOR THEIR DOMESTICATION IN SHINYANGA REGION, TANZANIA

|
|
An e-publication by the World Agroforestry Centre |
|
INDIGENOUS KNOWLEDGE OF
MEDICINAL TREES AND SETTING PRIORITIES |
|
|
Chapter 4 Openness of respondents Contrary to initial fears that it would not be easy to document knowledge on traditional medicine, most of the respondents turned out to be very open, with straightforward answers. Over 300 tree species were registered as medicinal plants (appendix 5). The local name, parts used and diseases treated were recorded for each tree mentioned by a respondent. Except on 2 occasions in Meatu and Bariadi, all respondents were eager to disclose medicinal details we felt were irrelevant to this study. The openness of respondents should put to rest the common myth that traditional healing is a secret.
Indigenous knowledge and participation by farmers was the underlying concept of this tree domestication programme. It was therefore essential to base this study on the experience and selection criteria of local people. One of the questions we used to provoke discussions in the field was, 'How did the people of this area treat diseases before the introduction of Western ideas on medicines?' The answers confirmed that rural people treasure an intimate knowledge of their environment, the trees around them and traditional ways of sustaining life with local resources. This knowledge, much of it inherited from past generations, is what we refer to as traditional or indigenous knowledge. Results from the investigation have established that the people of Shinyanga still rely heavily on over 300 tree species for treatment of a variety of diseases (appendix 5).
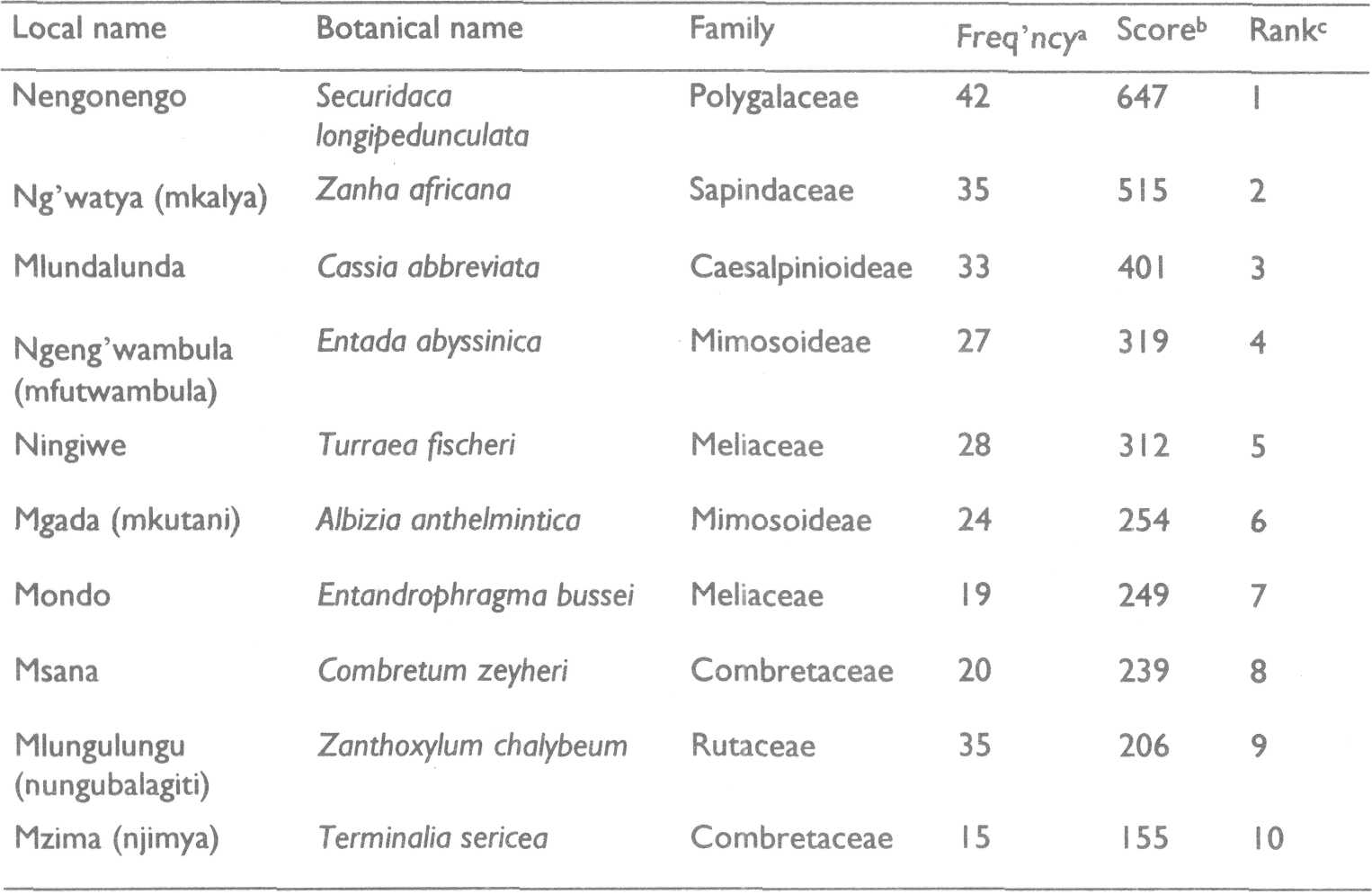
To set priorities on which of the medicinal trees to work on that the respondents identified was another major task. A prime candidate for domestication is a tree that scores high in priority hut is scarce in the area (Franzel and others 1996). The investigations revealed that the local people had used trees over generations for healing purposes. They had no doubt as to which of them were of greatest medicinal importance. The top 10 priority medicinal trees (PMTs) from all the data collected in the region are listed in table 4.1. Nengonengo, the local name for Securidaca longipedunculata, is without doubt the most sought-after medicinal tree. It tops the priority lists in nearly all the districts and user groups.
a Cumulative results from the number of times each tree
species was mentioned in all the interviews.
Of the 5 exotic species mentioned, only neem (Azadirachta indica) was ranked highly by both farmer and women's groups. Known globally as a medicinal tree and widely propagated in the region, the neem surprisingly rated only 13th in priority. This outcome raised many questions: Why was the neem tree so ignored by traditional healers? One traditional healer put it this way: 'My friend, this tree is like the chloroquine you buy in your drug stores. It was brought to us and we were told it cures 40 diseases, as its local name (mwarobaini) implies. They brought the seedlings free of charge and some people were even forced to plant them. Do you expect me to use something I don't know to treat my patients? No, no, no!' Practically all the tree seedlings one finds in the nurseries in the region are exotic species. Are development and extension agencies vigorously promoting the propagation of exotic tree species at the expense of more valuable and more valued indigenous species?
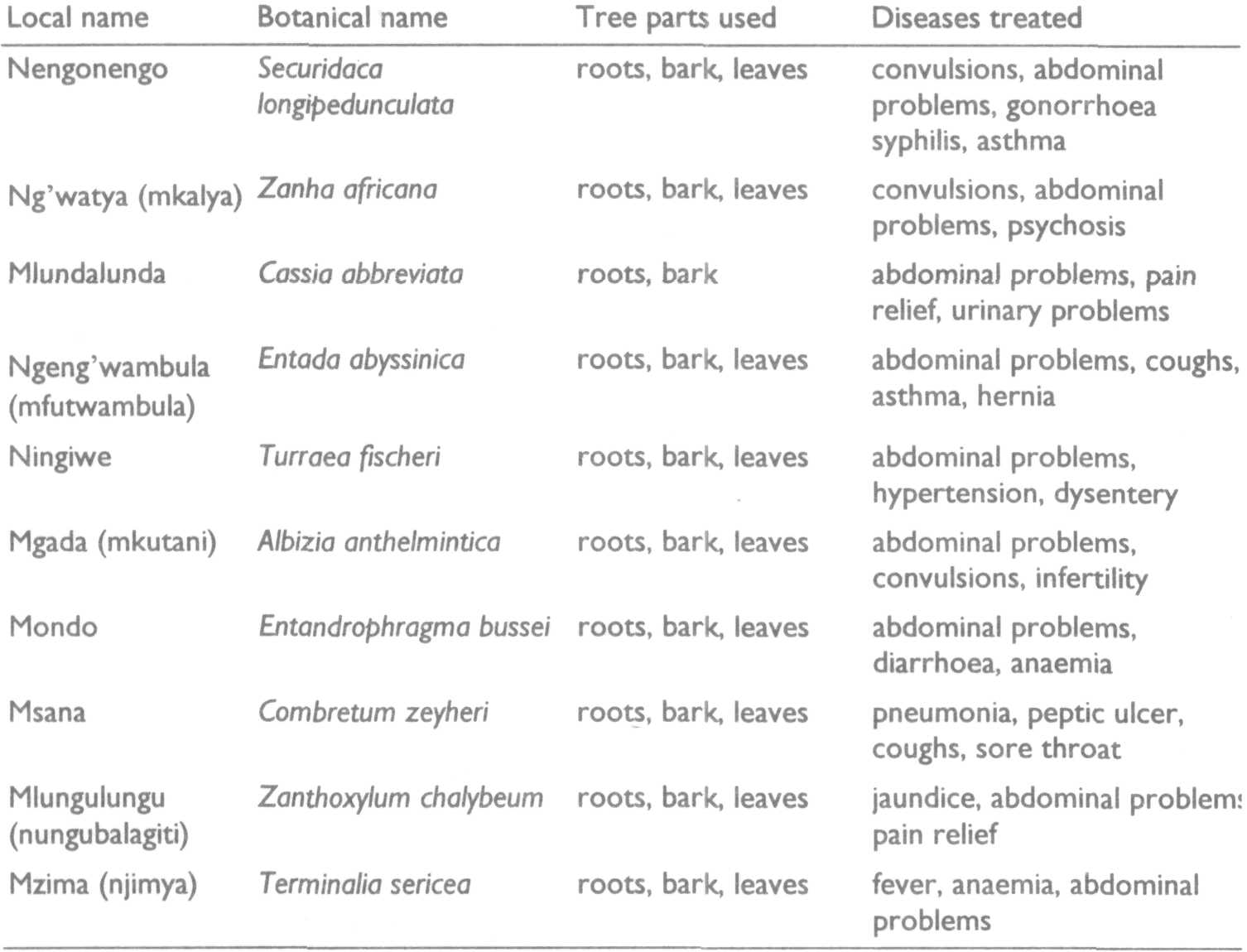
Results from the investigation have established that the people of Shinyanga still rely heavily on over 300 tree species for treatment of a variety of diseases. Tree parts reported to have medicinal properties were leaves, flowers, fruits, seeds, stem, wood, roots, even the whole tree in some cases. The root was the part used most frequently (appendix 5). Traditional healers said they peeled stem bark and excavated roots with great care so as not to kill the tree. The harvested parts that were not for immediate usage were usually cut into pieces and sun dried. The dry pieces were then stored by tying them into bundles and hanging them or by pounding them into powder and storing them in plastic or glass bottles, earth pots or gourds. If the parts were well stored, sellers and traditional healers claimed some remained potent for over a year. Over a hundred human diseases, including AIDS, were reported to be treated effectively with the medicinal trees named and listed (appendix 5). The fact that many traditional healers were eager to release such medicinal details was a great surprise. The most frequently mentioned ailments treated with parts of the PMTs are presented in table 4.2. How effective is traditional healing? Respondents had no doubt as to the potency of remedies made from PMTs. Cures from traditional healers are often made by mixing parts from several different trees. However, one must remember that to rural people 'medicine' reaches far beyond the tree parts used to treat a disease. Belief in the healer and the healing process is indispensable. We also emphasize that no claims are made as to the effectiveness of the treatments listed in this study. There is no doubt that some of these tree parts can be harmful, and idle experimentation could prove dangerous.
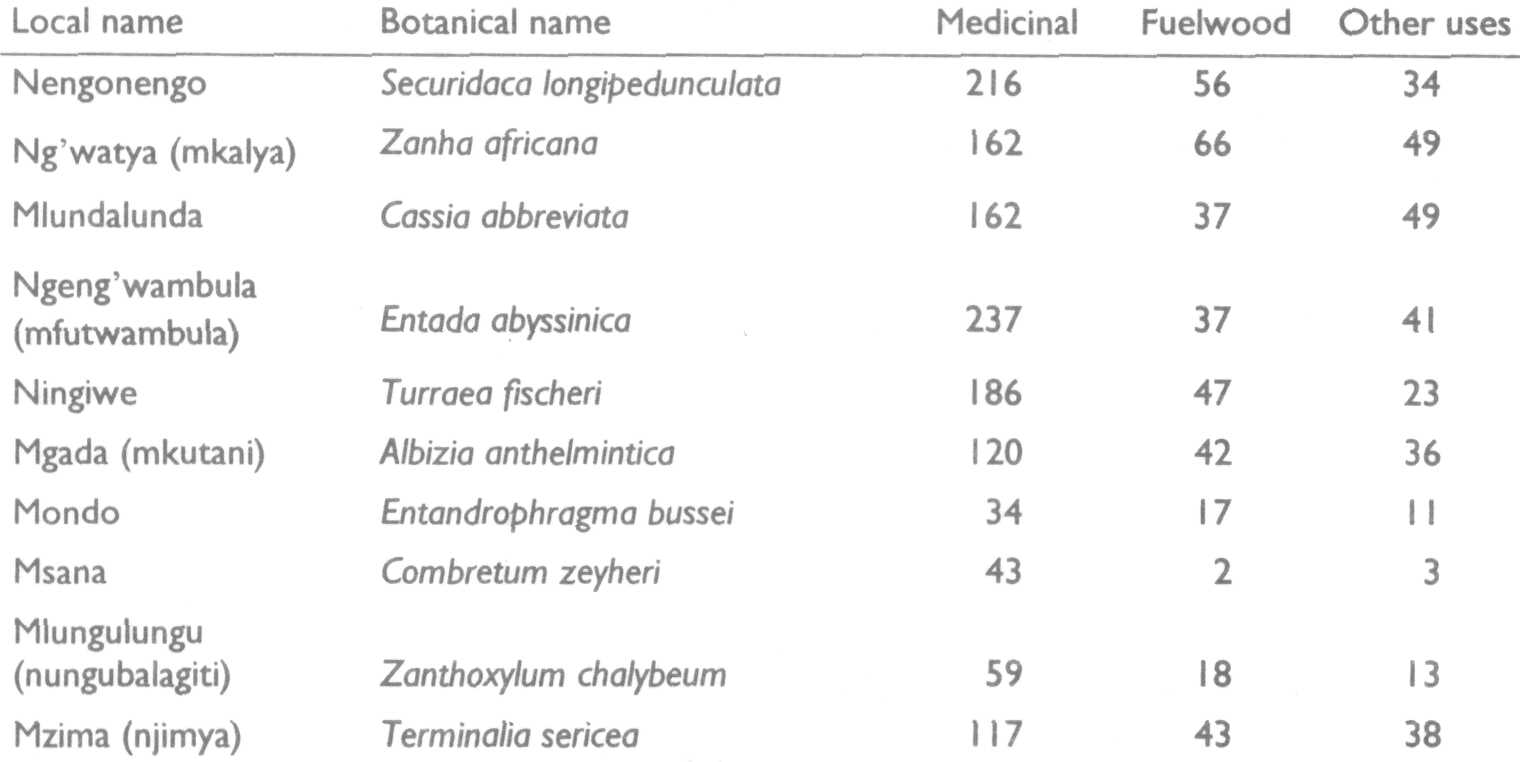
The PMTs also provide other useful products such as fuelwood, timber, construction poles and edibles. A single tree part can serve several purposes. Was it important to weigh the different uses? The main intention of domestication is to intensify the medicinal uses of the identified trees. Propagating a tree for medicinal purposes would be pointless if the species was valued immensely for fuelwood. Matrix scoring as described above under 'Participatory rural appraisal' was therefore used to further bring out what criteria respondents used in naming their priorities. The cumulative matrix scores for the PMTs are given in table 4.3. All the PMTs were preferred for their medicinal products.
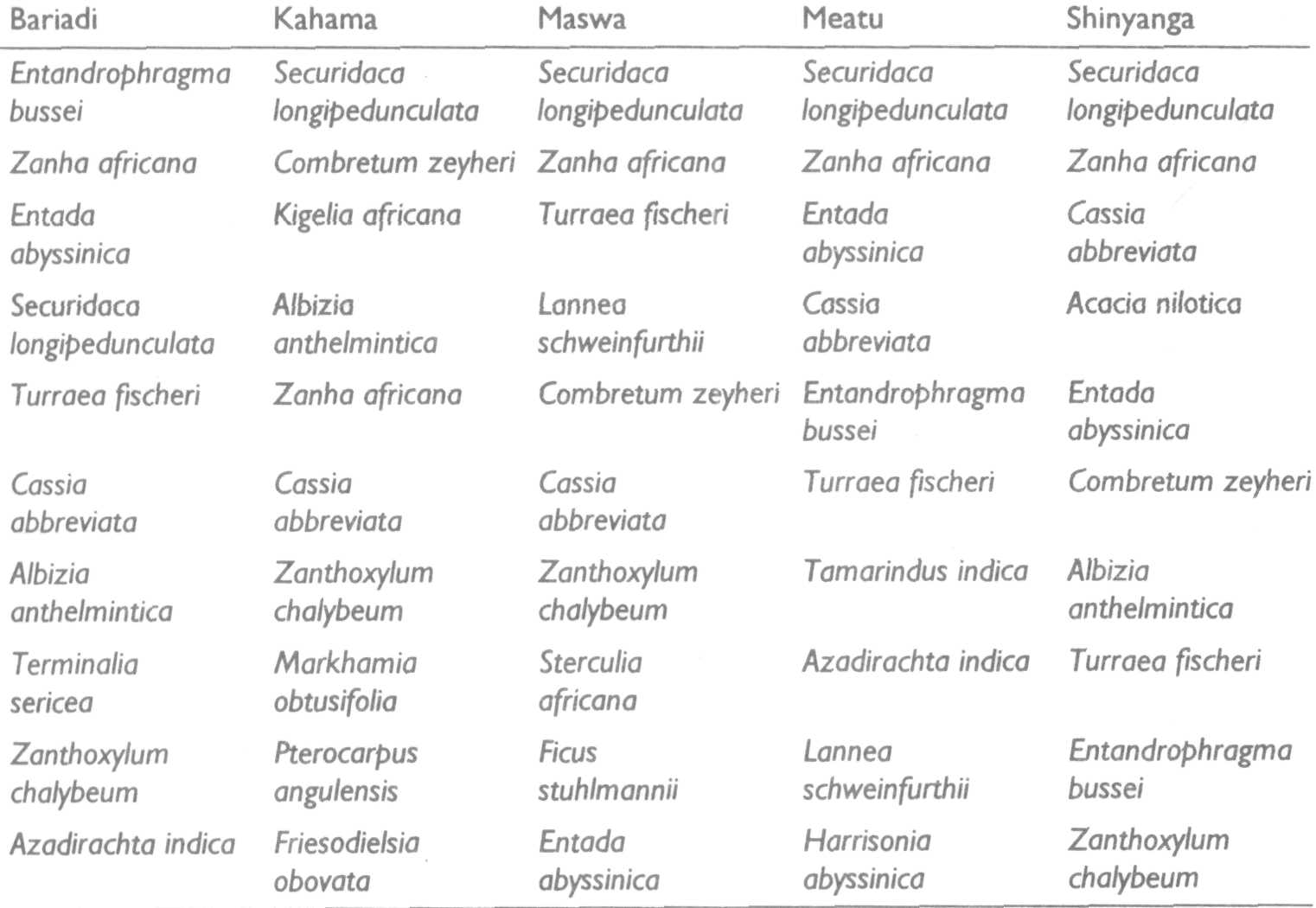
The districts are not uniform; they vary considerably in geography, environment and culture. This diversity called for resorting the data to determine the PMTs in each district. The results are given in table 4.4. How has human settlement influenced the vegetation in the region? As stated earlier, Shinyanga was said to have been extensively forested with woodland and bushland tree species (Otsyina 1992). The almost treeless open bush savannah covering much of the region is mainly from the combined influence of human and livestock populations (Maro 1995). The result of the tsetse fly eradication programme was a dramatic increase in human and livestock populations. Human activities such as clearing bush and forest for settlement, fuelwood and agriculture coupled with overgrazing by livestock have had profound effects on the environment. The region as a whole is faced with severe deforestation, leading to shortage of fuel, fodder and other tree products. The vegetation cover is denser in Kahama, where miombo woodlands still cover parts of the district.
'Food' rated no score for any PMT. Product preference of all PMTs was for medicine.
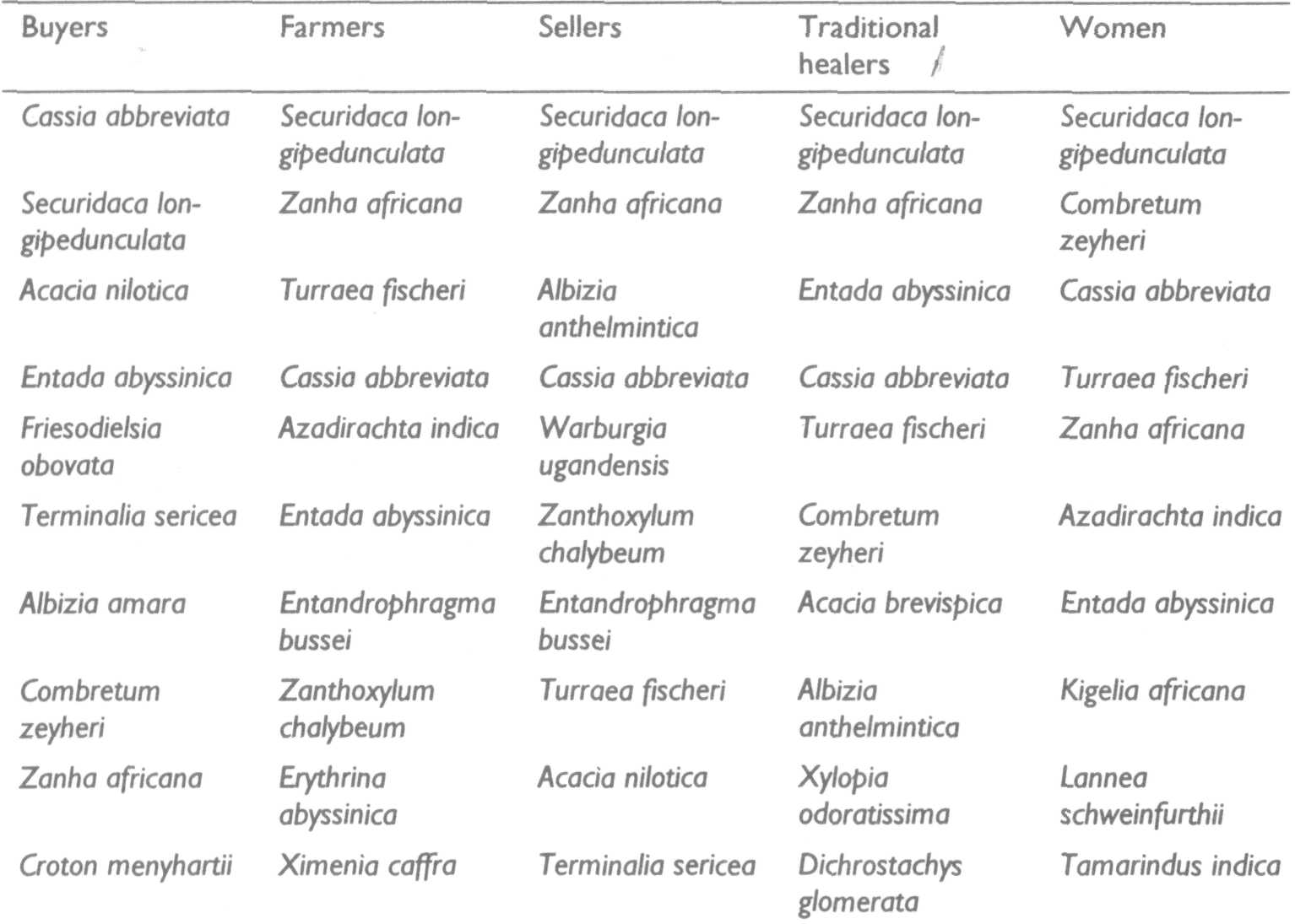
The identified user groups were indeed knowledgeable on medicinal trees. Many of the trees were mentioned repeatedly by all user groups. There was also little variation in the PMTs for each group (table 4.5). These independent results indicate that the PMTs must have some medicinal properties. Securidaca longipedunculata (nengonengo) is without doubt an important medicinal tree. Although virtually ignored by sellers and traditional healers, neem was quite popular among farmers and women's groups. Where are the healers and sellers of traditional medicine? There were at least 7 registered traditional healers in each of the villages we visited during the reconnaissance and PRA. Population estimates for these villages were between 500 and 2000 inhabitants. The traditional healer is still the only medical practitioner within reach of many rural people. One can hardly fail to find sellers of traditional medicine in all town centres and local markets in Shinyanga Region. Sellers from the Maasai tribe bring their medicines from outside the region. We could identify botanically very few of the Maasai medicinal trees.
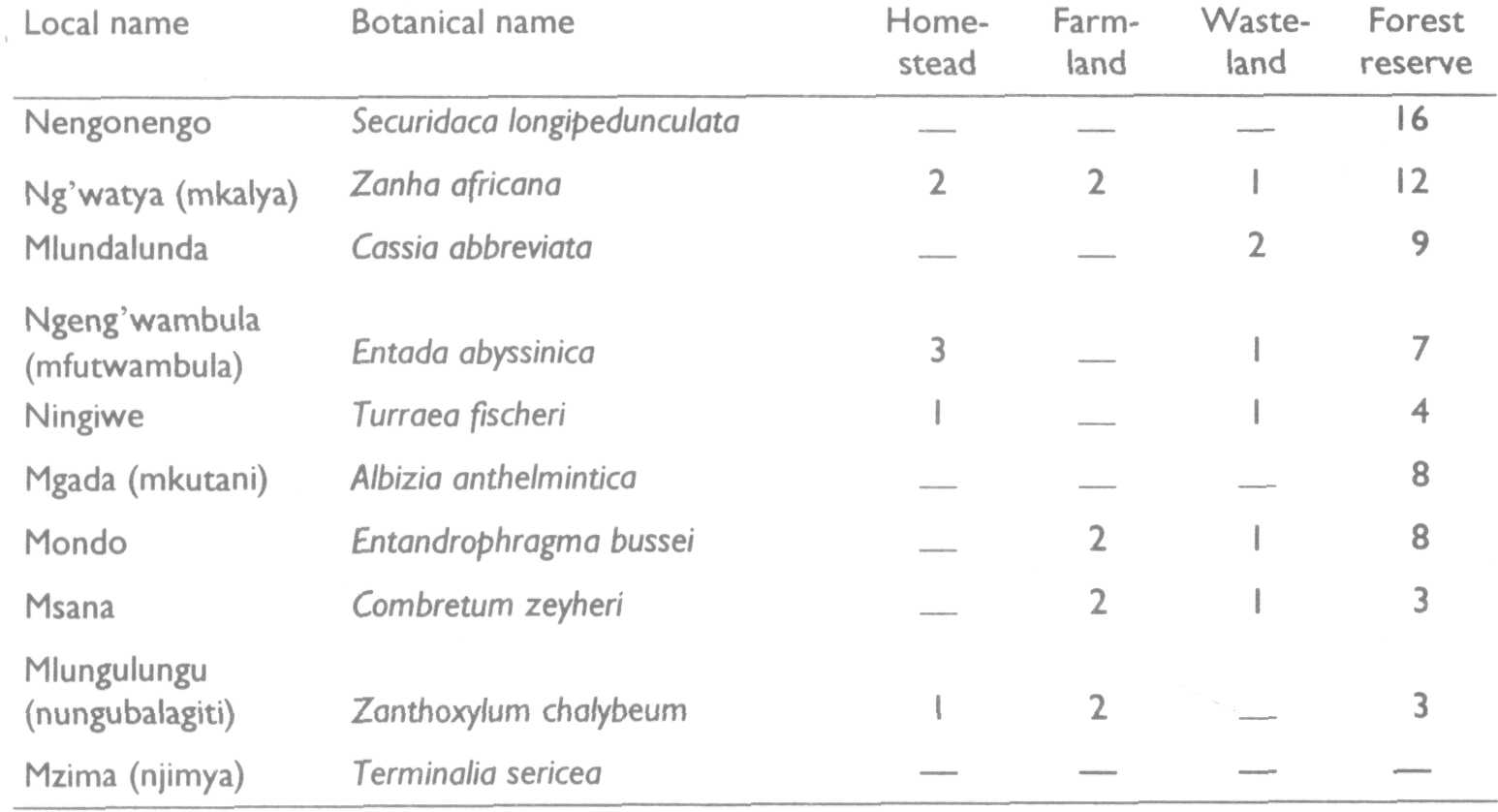
The urgency of domestication rests squarely on the medicinal value and availability status of the tree species. The first 7 PMTs were difficult to find in Kahama and extremely scarce in all the other districts. How is it that a popular tree like nengonengo is so scarce in 4 of the 5 districts? Has it never existed in these areas or has it been harvested to extinction? We got both yes and no answers to the latter question. An old man of about 70 years in Mwamishali village in Meatu District said the tree had been available in the village when he was a child. In Igaganulwa village in Bariadi District, another man about the same age said he had never seen the tree in his village. Could it have been harvested to extinction before he was born? It will be interesting to ascertain the truth in subsequent studies. The frequency count of PMT location is presented in table 4.6. Most PMTs are now found on uncultivated land, with the protected forest reserves as the main source of medicinal trees in the region. Respondents estimated the distances they had to travel to harvest priority medicinal tree parts. Among 63 respondents, 47 travelled farther than 10 km, 12 travelled up to 10 km, and only 4 travelled less than 1 km.
The long distances confirm the precarious status of PMTs in the region.
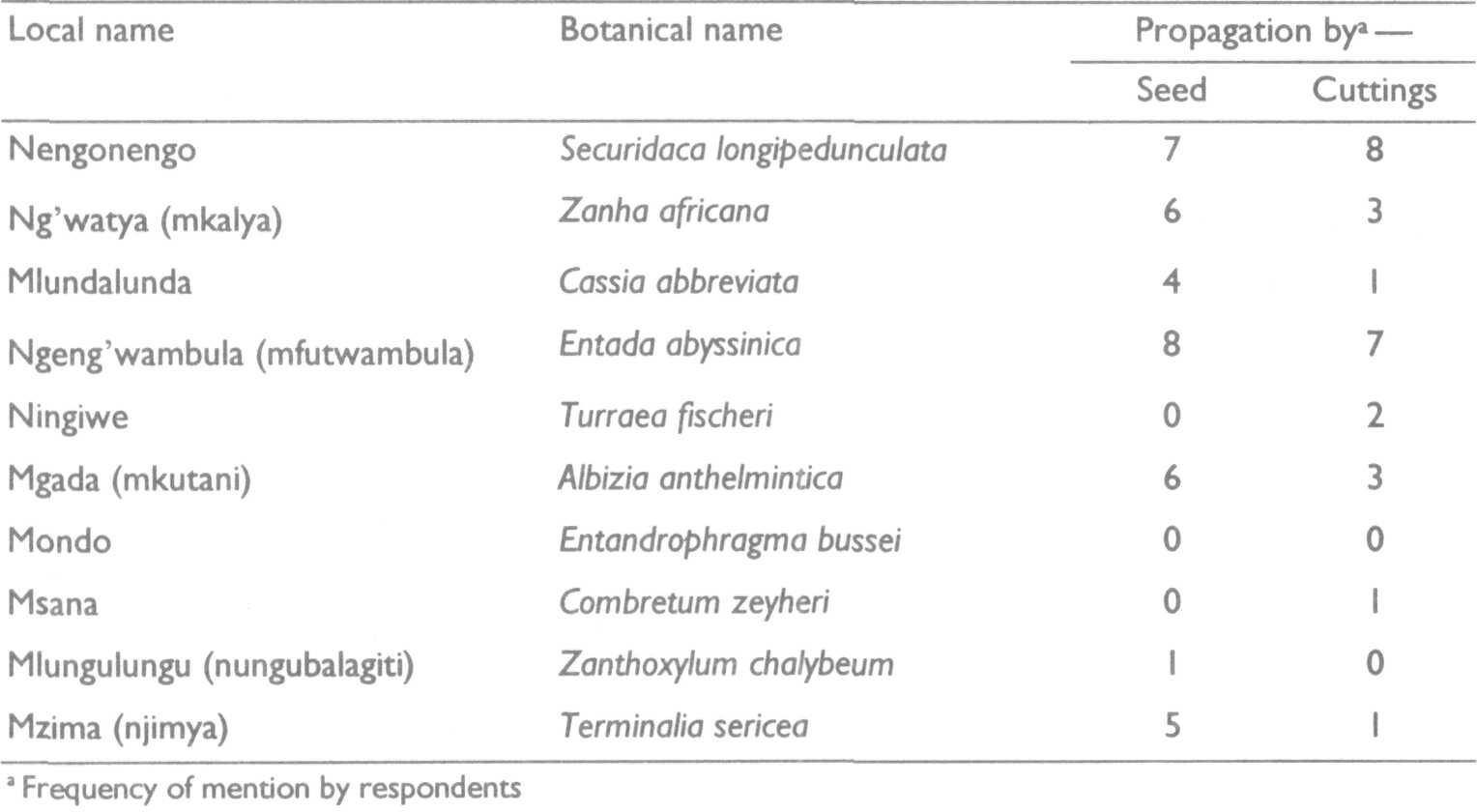
Respondents had intimate knowledge of the medicinal trees they listed. According to the information we gathered on ways to propagate them (table 4.7), it will be easy to propagate the first 4, while others like Combretum zeyheri may be difficult.
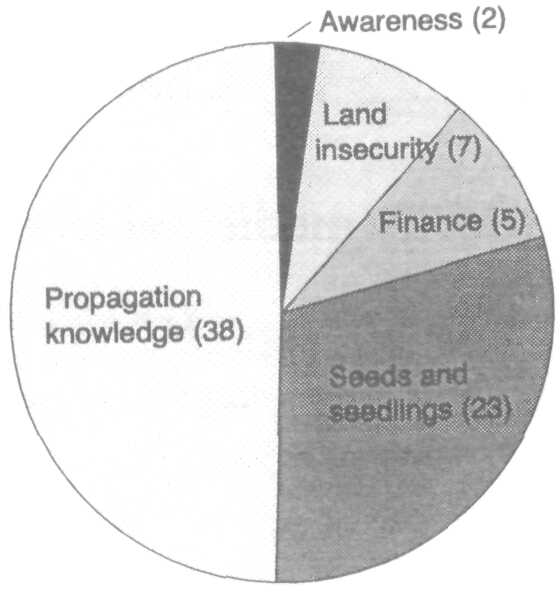
As respondents knew how to propagate some of the PMTs, what prevented them from propagating these trees in the past? Our findings are presented in figure 4.1. The overwhelming reason was the lack of skills to raise seedlings in a nursery. Most respondents also blamed the fact that seeds and seedlings were not available for sale (or for free). Few felt that money was a hindrance, and none mentioned labour as a problem. Some said that the lack of title to the land was a constraint.
To cross-check and consolidate the setting of priorities made earlier, we asked respondents towards the end of each interview to list the 3 medicinal tree species they would want most to plant on their farms. A combination of frequency count and scoring was used to rank these trees. The ranking for the first 10 positions was similar to that of table 4.1
Our ideas on domestication and conservation of medicinal trees were new to people in the 3 districts we first visited during the reconnaissance studies. This was not the case when we got to Maswa District. The district commissioner said we had come to steal an idea they had nourished for some time. The district cultural officer was more than delighted to discover new partners in a mission he had championed for the last several years. The chairman of the well-organized traditional healers' association could not believe they had finally found a mouthpiece to express what they had long been hoping for. In short, we were well received and felt at home with our ideas. The district cultural officer working with the traditional healers had already produced an inventory of medicinal plants in the district. In collaboration with the district authorities, primary schools and the HASHI/ ICRAF district office, they had initiated programmes to conserve and propagate some of the medicinal trees they had identified. We were shown 2 sites of approximately 8 and 12 hectares that they had been allocated for in situ conservation of medicinal plants. We were also taken to a nursery site they had acquired close to a water tank. We also visited a ward chairman who was one of the pioneers in promoting the cultivation of medicinal trees. He took us to parts of his farm he had earmarked for establishing medicinal gardens. We have much to learn from Maswa District and have yet to work out how best to collaborate with them. |